Abstract
Objective This study seeks to explore the association between common clinical indicators and pregnancy outcomes in patients with polycystic ovary syndrome (PCOS). Methods A cohort of 52 women with PCOS, 22 with isolated polycystic ovarian morphology (PCOM), 13 with isolated hyperandrogenism (HA), and 59 healthy controls was recruited from the Department of Reproductive Medicine, First Affiliated Hospital, Zhejiang University School of Medicine, between June 2021 and September 2022. Clinical parameters including age and body mass index (BMI) were recorded, while levels of D-dimer (DD), alanine aminotransferase (ALT), aspartate transaminase (AST), creatinine (Cr), urea nitrogen (UN), fasting plasma glucose (Glu), fasting insulin (Fins), and thyroid-stimulating hormone (TSH), embryo availability rate, fertilization Rate were measured. Differences across PCOS, PCOM, and HA groups were analyzed using analysis of variance and non-parametric tests. Results (1) In the PCOS group, significant differences were observed for embryo availability rate, age, WBC, TSH, ALT, AST, MAFLD, and BARD scores (P < 0.05). (2) Embryo availability was inversely associated with age, MAFLD, BARD, Fins, TSH, and WBC, and positively associated with AST (P < 0.05). (3) Fertilization rate was negatively correlated with V-PH, CA125, granulocyte percentage, BMI, Cr, and UN/Cr (P < 0.05). (4) ROC analysis of pregnancy outcomes in PCOS patients demonstrated that age, ALT, AST, AST/ALT, Cr, UN/Cr, DD, TSH, and CA125 had areas, sensitivities, and specificities above the moving average threshold. Conclusion Endocrine profiles differ significantly among PCOS, PCOM, and HA groups, and markers such as Age, ALT, AST, AST/ALT ratio, Cr, UN/Cr, DD, TSH, and CA125 can serve as potential predictors of pregnancy outcomes in patients with PCOS.
Keywords
Polycystic Ovary Syndrome, Pregnancy Outcomes, Clinical Indicators, Inflammation, Endocrine
1. Introduction
Polycystic ovary syndrome (PCOS) is a prevalent endocrine disorder associated with impaired female reproductive function. In addition to increasing the risk of cardiovascular disease and endometrial cancer
| [1] | Ioannis G, Lempesis, Samuel J, Apple, Gustavo, Duarte et al. Cardiometabolic effects of SGLT2 inhibitors on polycystic ovary syndrome. [J]. Diabetes Metab Res Rev, 2023, 39: e3634. https://doi.org/10.1002/dmrr.3634 |
[1]
in premenopausal women, PCOS has also been shown to significantly increase susceptibility of offspring to endocrine, neurological, and psychological disorders
| [2] | Anastasia, Trouva, Michael, Alvarsson, Jan, Calissendorff et al. Maternal thyroid function and offspring birth anthropometrics in women with polycystic ovary syndrome. [J]. Front Endocrinol (Lausanne), 2024, 15: 1343277.
https://doi.org/10.3389/fendo.2024.1343277 |
| [3] | Cesta CE, Öberg AS, Ibrahimson A, et al. Maternal polycystic ovary syndrome and risk of neuropsychiatric disorders in offspring: Prenatal androgen exposure or genetic confounding?. Psychol Med. 2020; 50(4): 616-624.
https://doi.org/10.1017/S0033291719000424 |
[2, 3]
. According to the National Health Service (NHS), PCOS is characterized by three diagnostic criteria: irregular menstruation, hyperandrogenism, and polycystic ovaries. Epidemiological data from China (2020)
| [4] | Wu Q, Gao J, Bai D, Yang Z, Liao Q. The prevalence of polycystic ovarian syndrome in Chinese women: A meta-analysis. Ann Palliat Med. 2021; 10(1): 74-87.
https://doi.org/10.21037/apm-20-1881 |
[4]
indicate that PCOS affects approximately 10% of women nationwide, with peak prevalence (17.23%) occurring in the 21–30-year age group. Emerging evidence suggests that the true incidence may be higher than currently estimated
. Women of reproductive age with PCOS frequently exhibit severe infertility and experience pronounced physiological disruptions, including menstrual irregularities, acne, hirsutism, and impaired psychological health
| [6] | Cotellessa L, Sobrino V, Silva MSB, et al. Preventing and correcting polycystic ovary syndrome by targeting anti-Müllerian hormone signaling in minipuberty and adulthood in mice. [J]. Cell Metab, 2025, 37(2): 248-262. e6.
https://doi.org/10.1016/j.cmet.2024.11.013 |
| [7] | Stener-Victorin E, Padmanabhan V, Walters KA, et al. Animal Models to Understand the Etiology and Pathophysiology of Polycystic Ovary Syndrome. [J]. Endocr Rev, 2020, 41(4): bnaa010. https://doi.org/10.1210/endrev/bnaa010 |
[6, 7]
. The multisystemic consequences of PCOS extend beyond individuals to families and subsequent generations, highlighting its significance as a public health priority. Accumulating studies suggest that dysregulated inflammatory signaling and endocrine dysfunction represent key pathological drivers of PCOS pathogenesis
| [8] | Fischer MB, Mola G, Rom AL, et al. Ovarian and Uterine Morphology in Minipuberty: Associations With Reproductive Hormones: a COPANA Study of 302 Girls. J Clin Endocrinol Metab. 2025; 110(4): 1015-1022.
https://doi.org/10.1210/clinem/dgad738 |
| [9] | Abbott DH, Levine JE, Dumesic PA, et al. POLYCYSTIC OVARY SYNDROME: ORIGINS AND IMPLICATIONS: Gestational anti-Müllerian hormone and testosterone excess combined with maternal adiposity program for polycystic ovary syndrome. [J]. Reproduction, 2025, 170(1): R1-R12.
https://doi.org/10.1530/REP-23-0548 |
[8, 9]
. Nevertheless, associations between routine clinical indicators of PCOS and disease severity/prognostic assessments remain underexplored. To address this gap, the present study examines correlations between standard clinical parameters and pregnancy outcomes in Chinese PCOS patients, to inform early clinical intervention strategies. The study protocol was approved by the Ethics Committee of the First Affiliated Hospital, Zhejiang University School of Medicine (Ethics Approval No. IIT20200672A).
2. Materials and Methods
2.1. Study Participants
This study recruited a total of 146 patients from the Reproductive Medicine Center, First Affiliated Hospital of Zhejiang University School of Medicine, who sought treatment between June 2021 and September 2022. Participants included the following groups:
1) Polycystic Ovary Syndrome (PCOS) Group: Fifty-two women diagnosed with PCOS, with a mean age of 30.06 years old, were selected. Diagnosis was established according to the 2003 Rotterdam criteria, requiring at least two of the following: (i) oligo-ovulation or anovulation; (ii) clinical or biochemical evidence of hyperandrogenism; and (iii) polycystic ovarian morphology, defined by the presence of ≥12 follicles measuring 2–9 mm in diameter in one or both ovaries and/or an ovarian volume ≥10 mL. Conditions associated with hyperprolactinemia and other sources of elevated androgens were excluded.
2) Polycystic Ovary Morphology (PCOM) Group: Twenty-two women with isolated PCOM were included, with an average age of 29.09 years old. Inclusion criteria were: (i) ovarian volume ≥10 mL (calculated as 0.5 × length × width × thickness in mm) and/or >12 follicles with a diameter of 2–9 mm per ovary; (ii) absence of hyperprolactinemia, irregular menstruation, elevated androgens, hypothalamic amenorrhea, and ovarian tumors.
3) Hyperandrogenic Anovulation (HA) Group: Thirteen women with hyperandrogenic anovulation, with a mean age of 30.85 years, were included. Inclusion criteria were: (i) serum testosterone >0.7 ng/mL (2.44 nmol/L) during the follicular phase of a regular cycle; (ii) maintenance of regular menstrual cycles; (iii) exclusion of medication-induced hyperandrogenism, polycystic ovarian morphology, endometriosis, disorders of sexual differentiation, and adrenal or ovarian testosterone secretion abnormalities.
4) Control Group: Fifty-nine healthy women with a mean age of 28.86 years old served as controls. Inclusion criteria included: (i) regular menstrual cycles; (ii) absence of polycystic ovarian morphology; (iii) no hormonal abnormalities such as hyperandrogenism; and (iv) no ovarian, tubal, or uterine disorders.
All participants underwent ovarian stimulation using a GnRH antagonist protocol. Hematological, liver, kidney, and lipid profiles were within normal ranges, and participants had no history of liver, kidney, hypothalamic, or other relevant systemic diseases. Exclusion criteria for all groups included hyperprolactinemia, congenital adrenal hyperplasia, Cushing's syndrome, ovarian or adrenal disease, Sjögren’s syndrome, systemic lupus erythematosus, thyroid dysfunction, diabetes, endocrine-related conditions, genetic disorders, and recent use of endocrine-modulating drugs (within the three months prior to study participation). The study protocol was approved by the Ethics Committee of Zhejiang University School of Medicine.
2.2. Observation Indicators
1) General Indicators
Age, height, and weight were measured for all subjects, and Body Mass Index (BMI) was calculated as weight (kg) divided by square of height (m2).
2) Inflammatory Markers
Inflammatory markers measured included white blood cell count (WBC), absolute neutrophil count (Granulocyte), neutrophil percentage (Gran%), and erythrocyte sedimentation rate (ESR).
3) Endocrine and Metabolic Markers
Fasting plasma glucose (Glu), fasting insulin (Fins), thyroid-stimulating hormone (TSH), alanine aminotransferase (ALT), aspartate transaminase (AST), MAFLD score, HIS score, BARD score, urea nitrogen (UN), serum creatinine (Cr), D-dimer (DD), and vaginal pH (V-PH) were assessed.
The scores were calculated as follows:
MAFLD score = -2.89 + 1.18 × metabolic syndrome (1 = diagnosed, 0 = excluded) + 0.45 × type 2 diabetes (1 = diagnosed, 0 = excluded) + 0.15 × Fins (mU/L) + 0.04 × AST (U/L) - 0.94 × AST/ALT (U/L).
HIS score = 8 × ALT/AST (U/L) + BMI (kg/m2) + 2 + 2 × type 2 diabetes (1 = diagnosed, 0 = excluded).
BARD score = BMI (kg/m2) + type 2 diabetes (1 = diagnosed, 0 = excluded) + 2 × ALT/AST (U/L) (1 = diagnosed, 0 = excluded).
4) Reproductive Outcome Indicators
Fertilization rate was calculated as the ratio of fertilized eggs to mature follicles, and high-quality embryo rate was determined as the proportion of embryos graded B+ or higher on day 3 relative to the total number of fertilized eggs.
2.3. Statistical Methods
Statistical analyses were conducted using SPSS software, version 26.0. Tests for normality and homogeneity of variance were applied to all quantitative variables. Data with normal distributions are presented as mean ± standard deviation (x ± s), while non-normally distributed data were analyzed with the Kruskal-Wallis non-parametric test. Pearson’s correlation analysis was used to assess relationships between variables. Receiver Operating Characteristic (ROC) curve analysis was conducted to evaluate the diagnostic efficacy of clinical indicators in predicting pregnancy outcomes in PCOS, with Youden’s Index (YI) calculated to identify optimal cutoff values. A significance threshold of P < 0.05 was applied throughout.
3. Results
3.1. Baseline Characteristics and Mean Values of Indicators Among PCOS, PCOM, HA, and Control Groups
Baseline characteristics and mean values for key indicators across the PCOS, PCOM, HA, and control groups were summarized in
Table 1. Significant differences were observed between the PCOS and control groups in high-quality embryo rate, age, WBC count, TSH, ALT, AST, MAFLD score, and BARD score (P < 0.05). Additionally, the PCOM group demonstrated significant differences compared to controls in high-quality embryo rate, fasting insulin (Fins), MAFLD score, and HIS score (P < 0.05). No statistically significant differences were observed between the HA and control groups (P value > 0.05).
Table 1. Comparison of General Characteristics and Laboratory Indicators among.
Group | Control (n=59) | PCOS (n=52) | P value | PCOM (n=22) | P value | HA (n=13) | P value |
Mean | Mean | Mean | Mean |
Embryo Rate | 0.44±0.04 | 0.39±0.03 | 0.01* | 0.39±0.06 | 0.01* | 0.47±0.07 | 0.36 |
Fertilization Rate | 0.51±0.04 | 0.49±0.04 | 0.52 | 0.36±0.08 | 0.13 | 0.64±0.09 | 0.26 |
Age | 28.86±0.52 | 30.06±0.59 | 0.002* | 29.09±0.75 | 0.43 | 30.85±0.95 | 0.42 |
BMI | 22.83±0.46 | 23.81±0.50 | 0.03* | 24.31±0.82 | 0.11 | 21.12±0.77 | 0.11 |
ALT | 16.64±1.54 | 23.42±3.35 | 0.02* | 24±6.24 | 0.10 | 21.25±3.41 | 0.22 |
AST | 17.67±0.77 | 22.96±2.53 | 0.02* | 20.63±2.1 | 0.11 | 20±1.5 | 0.20 |
AST/LT | 1.23±0.06 | 1.14±0.06 | 0.22 | 1.14±0.2 | 0.53 | 1.13±0.13 | 0.46 |
Cr | 57.26±1.30 | 57.34±1.19 | 0.91 | 57.06±2.6 | 0.94 | 54.33±1.46 | 0.32 |
UN/Cr | 78.95±2.51 | 73.15±2.66 | 0.24 | 70.60±4.9 | 0.12 | 83.04±4.38 | 0.49 |
V-PH | 4.03±0.06 | 3.96±0.05 | 0.60 | 4.01±0.11 | 0.92 | 3.8±0 | 0.09 |
Fins | 6.0±0.5 | 11.30±1.57 | 0.001* | 12.06±4.69 | 0.01* | 6.98±2.40 | 0.54 |
D-D· | 268.79±18.57 | 285.13±22.15 | 0.27 | 249.25±25.17 | 0.56 | 303.7±61.75 | 0.47 |
ESR | 7.25±0.5 | 8.95±0.85 | 0.09 | 8.94±1.10 | 0.13 | 8.2±1.07 | 0.46 |
TSH | 2.28±0.17 | 1.83±0.14 | 0.01* | 1.79±0.25 | 0.16 | 2.26±0.60 | 0.98 |
WBC | 6.40±0.30 | 7.17±0.28 | 0.02* | 7.26±0.31 | 0.12 | 6.98±0.76 | 0.44 |
Gran% | 60.60±1.27 | 59.81±1.41 | 0.78 | 62.4±1.98 | 0.46 | 59.1±2.30 | 0.62 |
Gran | 4.07±0.27 | 4.32±0.22 | 0.16 | 4.74±0.32 | 0.18 | 4.24±0.60 | 0.80 |
CA125 | 22.65±1.90 | 19.86±2.02 | 0.24 | 19.90±2.17 | 0.43 | 26.18±7.35 | 0.52 |
MAFLD | -2.63±0.75 | -2.29±0.76 | 0.002* | -2.31±0.47 | 0.004* | -2.63±0.92 | 0.41 |
HIS | 34.02±3.75 | 34.24±5.52 | 0.39 | 34.02±3.75 | 0.027* | 31.81±3.02 | 0.28 |
BARD | 24.24±3.40 | 25.08±5.57 | 0.045* | 24.95±6.76 | 0.067 | 22.84±3.14 | 0.91 |
Gran% represents the percentage of neutrophils relative to the total white blood cell count, while Gran denotes the absolute neutrophil count. Asterisks (*) indicate statistical significance at P < 0.05.
To assess potential inter-group differences in baseline values of clinical indicators, a Kruskal-Wallis test was performed. The analysis revealed significant inter-group differences in aspartate transaminase (AST), fasting insulin (Fins), and white blood cell count (WBC) (H-values = 11.303, 18.219, and 11.128, respectively; P < 0.05). No statistically significant differences were found for other indicators, including age., BMI, erythrocyte sedimentation rate (ESR), neutrophil percentage (Gran%), absolute neutrophil count (Gran), thyroid-stimulating hormone (TSH), alanine aminotransferase (ALT), AST/ALT ratio, creatinine (Cr), urea nitrogen/creatinine ratio (UN/Cr), vaginal pH (V-PH), D-dimer (DD), cancer antigen 125 (CA125), MAFLD score, HIS score, BARD score, high-quality embryo rate, and fertilization rate (H-values = 3.435, 1.093, 2.642, 1.157, 7.533, 5.051, 6.682, 3.506, 2.152, 5.318, 4.482, 0.365, 2.725, 0.181, 5.625, 5.722, 1.503, 5.619; all P > 0.05). These findings suggest that insignificant baseline differences between groups minimized potential confounding effects with age, BMI, ESR, Gran%, Gran, TSH, ALT, AST/ALT ratio, Cr, UN/Cr, V-PH, DD, CA125, MAFLD score, HIS score, BARD score, high-quality embryo rate, and fertilization rate.
3.2. Further Inter-group Comparative Analysis
1) AST Level Comparisons
After comparison with the control group, significant elevations in aspartate transaminase (AST) levels were observed in both the PCOS and PCOM groups, as well as the HA group, with H-values of -18.884, -25.328, and -23.213, respectively (all P < 0.05). No significant differences were observed in the remaining inter-group comparisons (all P > 0.05).
2) Fasting Insulin Comparisons
The PCOS group exhibited significantly increase in fasting insulin levels in comparison to the control group, with an H-value of -26.269 (P < 0.05). However, no significant differences were observed among the other inter-group comparisons (all P > 0.05).
3) WBC Count Comparisons
Significant increases in white blood cell (WBC) counts were noted in comparisons between the PCOS and PCOM groups with the control group, with H-values of -20.842 and -26.452, respectively (both P < 0.05). No statistical disparities between the HA group and the control group, nor among the PCOS, PCOM, and HA groups (all P > 0.05).
3.3. Correlation Analysis of Pregnancy Outcomes and Clinical Indicators
Pearson correlation analysis revealed significant negative correlations between the good embryo rate and age, MAFLD score, BARD score, fasting insulin (Fins), thyroid-stimulating hormone (TSH), and white blood cell (WBC) count, with correlation coefficients (r) of -0.201, -0.463, -0.514, -0.488, -0.230, and -0.263, respectively (all P < 0.05). Conversely, the good embryo rate exhibited a significant positive correlation with AST, with an r value of 0.879 (P < 0.05). Furthermore, the fertilization rate demonstrated significant negative correlations with vaginal pH (V-PH), cancer antigen 125 (CA125), neutrophil percentage (Gran%), body mass index (BMI), creatinine (Cr), and urea nitrogen/creatinine ratio (UN/Cr), with r values of -0.355, -0.184, -0.183, -0.894, -0.188, and -0.223, respectively (P < 0.05) (
Table 2).
Table 2. Correlation of Pregnancy Outcomes with Common Clinical Indicators.
Bivariate Analysis | Pearson Correlation Coefficient | P-value |
High-quality embryo rate -Age | -0.201 | 0.026 |
High-quality embryo rate -AST | 0.879 | 0.000 |
High-quality embryo rate -MAFLD | -0.463 | 0.000 |
High-quality embryo rate -BARD | -0.514 | 0.000 |
High-quality embryo rate -FIN | -0.488 | 0.000 |
High-quality embryo rate -TSH | -0.230 | 0.011 |
High-quality embryo rate -WBC | -0.263 | 0.022 |
High-quality embryo rate -V-PH | -0.355 | 0.000 |
High-quality embryo rate -CA125 | -0.184 | 0.0455 |
High-quality embryo rate -Gran% | -0.183 | 0.040 |
High-quality embryo rate -BMI | -0.894 | 0.000 |
High-quality embryo rate -Cr | -0.188 | 0.039 |
High-quality embryo rate -UN/Cr | -0.223 | 0.014 |
3.4. Diagnostic Value of Common Clinical Indicators in Relation to Pregnancy Outcomes in PCOS Patients
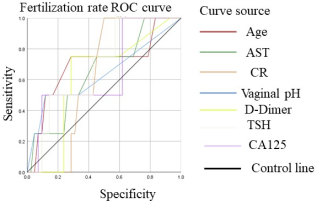
To assess the diagnostic value of the fertilization rate in conjunction with common clinical indicators, receiver operating characteristic (ROC) curve analysis was conducted. Indicators with an area under the curve (AUC) greater than 50% included age, alanine aminotransferase (ALT), aspartate transaminase (AST), AST/ALT ratio, creatinine (Cr), urea nitrogen/creatinine ratio (UN/Cr), vaginal pH (V-PH), D-dimer (D-D), thyroid-stimulating hormone (TSH), and cancer antigen 125 (CA125). Among these, age, AST, Cr, V-PH, D-D, TSH, and CA125 exhibited AUC values exceeding 60%, specifically 69.9%, 64.9%, 61.9%, 63.7%, 61.9%, 64.9%, and 69.0%, respectively.
To refine the optimal threshold values for clinical diagnosis and to further explore the diagnostic significance of these indicators in relation to the fertilization rate in PCOS patients, the Youden indices for Age, ALT, AST, AST/ALT, Cr, UN/Cr, V-PH, D-D, TSH, and CA125 were calculated as follows: 30.50 (YI = 0.47), 24.50 (YI = 0.33), 17.50 (YI = 0.30), 1.15 (YI = 0.32), 56.50 (YI = 0.50), 68.74 (YI = 0.20), 4.70 (YI = 0.38), 289.00 (YI = 0.46), 3.83 (YI = 0.41), and 12.65 (YI = 0.29), respectively (
Figure 1).
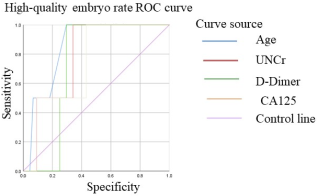
To ascertain the diagnostic value of the good embryo rate in relation to prevalent clinical indicators, receiver operating characteristic (ROC) curve analysis was conducted. The indicators with an area under the curve (AUC) exceeding 50% included age, alanine aminotransferase (ALT), aspartate transaminase (AST), AST/ALT ratio, creatinine (Cr), urea nitrogen/creatinine ratio (UN/Cr), D-dimer (D-D), thyroid-stimulating hormone (TSH), and cancer antigen 125 (CA125). Notably, age, UN/Cr, D-D, and CA125 demonstrated AUC values surpassing 70%, specifically 85.2%, 78.4%, 72.7%, and 73.9%, respectively.
Figure 1. Fertilization rate ROC curve (area under the line > 60%).
To refine the optimal threshold values for the clinical diagnosis and to further investigate the diagnostic significance of these common clinical indicators associated with the good embryo rate in in individuals diagnosed with polycystic ovary syndrome (PCOS), the Youden indices for age, ALT, AST, AST/ALT, Cr, UN/Cr, D-D, TSH, and CA125 were calculated as follows: 30.50 (YI = 0.71), 12.50 (YI = 0.39), 32.50 (YI = 0.46), 1.15 (YI = 0.57), 56.50 (YI = 0.48), 75.78 (YI = 0.66), 289.00 (YI = 0.71), 4.58 (YI = 0.43), and 17.85 (YI = 0.57), separately (
Figure 2).
Figure 2. High-quality embryo rate ROC curve (area under the line >70%).
4. Discussion
Polycystic ovary syndrome (PCOS) is a common hormonal condition in women of reproductive age, marked by elevated androgen levels, irregular menstrual cycles, and the polycystic ovaries. Beyond its role in causing persistent anovulation and reproductive dysfunction, PCOS significantly increases the risk of various metabolic disorders, including hirsutism and acne attributable to elevated androgen levels, type 2 diabetes linked to impaired glucose metabolism, obesity and hyperlipidemia stemming from abnormal lipid metabolism, and the development of metabolic syndrome.
Previous studies have identified chronic low-grade inflammation and dysregulated lipid metabolism as critical risk factors contributing for reproductive impairments in women with PCOS
| [9] | Abbott DH, Levine JE, Dumesic PA, et al. POLYCYSTIC OVARY SYNDROME: ORIGINS AND IMPLICATIONS: Gestational anti-Müllerian hormone and testosterone excess combined with maternal adiposity program for polycystic ovary syndrome. [J]. Reproduction, 2025, 170(1): R1-R12.
https://doi.org/10.1530/REP-23-0548 |
| [10] | Joham AE, Norman RJ, Stener-Victorin E, et al. Polycystic ovary syndrome. Lancet Diabetes Endocrinol. 2022; 10(9): 668-680. https://doi.org/10.1016/S2213-8587(22)00163-2 |
[9, 10]
. Notably, current research predominantly emphasizes the molecular mechanisms of PCOS at genetic, hormonal, and endocrine levels
| [11] | di Clemente N, Racine C, Pierre A, et al. Anti-Müllerian Hormone in Female Reproduction. [J]. Endocr Rev, 2021, 42(6): 753-782. https://doi.org/10.1210/endrev/bnab012 |
| [12] | Dapas M, Dunaif A. Deconstructing a Syndrome: Genomic Insights Into PCOS Causal Mechanisms and Classification. [J]. Endocr Rev, 2022, 43(6): 927-965.
https://doi.org/10.1210/endrev/bnac001 |
| [13] | Kazemi M, Kim JY, Wan C, et al. Comparison of dietary and physical activity behaviors in women with and without polycystic ovary syndrome: a systematic review and meta-analysis of 39 471 women. [J]. Hum Reprod Update, 2022, 28(6): 910-955. https://doi.org/10.1093/humupd/dmac023 |
| [14] | Geng L, Yang X, Sun J, et al. Gut Microbiota Modulation by Inulin Improves Metabolism and Ovarian Function in Polycystic Ovary Syndrome. [J]. Adv Sci (Weinh), 2025, 12(8): e2308401. https://doi.org/10.1002/advs.202308401 |
[11-14]
, while the clinical assessment using relevant indicators remains underexplored. Consequently, few analyses from a clinical perspective that utilize commonly encountered clinical indicators to evaluate pregnancy outcomes in PCOS.
Our study bridges this gap using normal reproductive-age women as a control group. By comparing inflammatory and related endocrine indicators among patients with PCOS, pure polycystic ovary morphology (PCOM), and pure hyperandrogenism (HA), we controlled confounding effects associated with isolated ovarian cyst-like changes and isolated elevated androgen levels. This methodological approach allowed for a more precise identification of differences in inflammatory and endocrine indicators among the groups. The findings indicate statistically significant differences in these indicators, suggesting that serum inflammatory and related endocrine markers may thus serve as predictors for PCOS pregnancy outcomes.
4.1. PCOS Lipid Metabolism
Patients with PCOS exhibit ~2× higher obesity rates versus controls
. Our data showed a notable variation in body mass index (BMI) values between the PCOS group and the control group. Previous researches
| [12] | Dapas M, Dunaif A. Deconstructing a Syndrome: Genomic Insights Into PCOS Causal Mechanisms and Classification. [J]. Endocr Rev, 2022, 43(6): 927-965.
https://doi.org/10.1210/endrev/bnac001 |
| [13] | Kazemi M, Kim JY, Wan C, et al. Comparison of dietary and physical activity behaviors in women with and without polycystic ovary syndrome: a systematic review and meta-analysis of 39 471 women. [J]. Hum Reprod Update, 2022, 28(6): 910-955. https://doi.org/10.1093/humupd/dmac023 |
[12, 13]
has suggested that obesity constitutes a major contributing factor for diagnosing PCOS in females of pre-reproductive age. Monitoring and controlling BMI in adolescent females who exceed the highest threshold of the normal range may mitigate the risk of developing PCOS.
Moreover, a meta-analysis
| [14] | Geng L, Yang X, Sun J, et al. Gut Microbiota Modulation by Inulin Improves Metabolism and Ovarian Function in Polycystic Ovary Syndrome. [J]. Adv Sci (Weinh), 2025, 12(8): e2308401. https://doi.org/10.1002/advs.202308401 |
| [15] | Martínez-García MÁ, Luque-Ramírez M, San-Millán JL, et al. Body iron stores and glucose intolerance in premenopausal women: role of hyperandrogenism, insulin resistance, and genomic variants related to inflammation, oxidative stress, and iron metabolism. [J]. Diabetes Care, 2009, 32(5): 934-936. https://doi.org/10.2337/dc08-1962 |
| [16] | Chen YH, Heneidi S, Lee JM, et al. miRNA-93 inhibits GLUT4 and is overexpressed in adipose tissue of polycystic ovary syndrome patients and women with insulin resistance. Diabetes. 2013; 62(7): 2278-2286.
https://doi.org/10.2337/db12-0963 |
[14-16]
shows that overweight or obese women with PCOS prior to reproduction face more severe metabolic disorders compared to those with a normal BMI. In our study, we categorized participants into three BMI groups: underweight (BMI < 20), normal weight, and overweight (BMI > 25) and examined potential differences in pregnancy outcomes, specifically fertilization rates and good embryo rates. Our results showed no meaningful statistical variations between these groups (P > 0.05; this analysis is not displayed in this paper). However, we identified correlations between indicators of liver and bile metabolism, such as alanine aminotransferase (ALT), aspartate transaminase (AST), and fasting insulin (FIN), and pregnancy outcomes.
Prior research suggests that these correlations may be linked to impaired mechanisms of insulin receptor tyrosine phosphorylation within adipocytes of PCOS patients, which leads to significant functional abnormalities. For instance, a reduction is observed in the ability of adipose tissue to undergo lipolysis and respond to insulin, along with abnormal secretion of adipokines and diminished glucose uptake by adipocytes. Furthermore, mechanistic studies have demonstrated that dysfunctional adipose tissue contributes to elevated levels of free fatty acids (FFAs), promoting insulin resistance, lipid dysregulation, and metabolic syndrome, ultimately resulting in liver function and glucose metabolism abnormalities. These findings align with our Section 2.2 results.
4.2. PCOS Chronic Inflammation
Elevated expression of inflammatory factors correlates with reproductive impairments in patients with polycystic ovary syndrome (PCOS). A substantial body of evidence shows that levels of high-sensitivity C-reactive protein (hsCRP), interleukin-1 beta (IL-1β), interleukin-18 (IL-18), and white blood cell (WBC) counts are significantly increased in PCOS patients
| [17] | Ambikairajah A, Walsh E, Tabatabaei-Jafari H, Cherbuin N. Fat mass changes during menopause: a meta-analysis. Am J Obstet Gynecol. 2019; 221(5): 393-409.
https://doi.org/10.1016/j.ajog.2019.04.023 |
| [18] | Xiao Peng, Ren Jingjing, Yao Lingnu, et al. Longitudinal study of chronic low-grade inflammatory response in polycystic ovary syndrome: preliminary compilation and analysis of inflammation and related endocrine risk indicators [J]. General Practice Clinical and Education, 2021, 19(02): 102-107. |
[17, 18]
. These results are consistent with our study, which found WBC counts negatively correlate with embryo quality rates, as well as a significant inverse association between fertilization rates and granulocyte percentage (Gran%). (as detailed in Section 2.2).
The mechanism through which systemic inflammatory responses lead to adverse pregnancy outcomes in PCOS patients may be associated with macrophages, key immune cells that serve a pivotal function in the inflammatory process. Macrophages are among the most abundant immune cells present in the tissue microenvironment under various pathological conditions, including PCOS, and act as a key source of inflammatory mediators such as tumor necrosis factor-alpha (TNF-α), interleukin-6 (IL-6), and C-C motif chemokine ligand 2 (CCL2). The equilibrium between M1 (pro-inflammatory) and M2 (anti-inflammatory) macrophages is essential in shaping both physiological and pathological processes
| [19] | Torstensson S, Ascani A, Risal S, et al. Androgens Modulate the Immune Profile in a Mouse Model of Polycystic Ovary Syndrome. [J]. Adv Sci (Weinh), 2024, 11(5): e2304470.
https://doi.org/10.1002/advs.202304470 |
[19]
. Elevated androgen levels have been shown to increase the population of ovarian M1 macrophages, which express chemokine-like receptors and stimulate the secretion of various inflammatory factors, including TNF-α, IL-6, inducible nitric oxide synthase (iNOS), IL-12, and IL-1β, while simultaneously inhibiting the expression of IL-10. This shift drives macrophages from the anti-inflammatory M2 phenotype toward the pro-inflammatory M1 phenotype
.
In addition to macrophages, granulosa cells act as a key role in the ovarian inflammatory cellular environment. These cells provide approximately 85% of the nutritional support to oocytes, with their growth and development directly influencing follicle initiation, maturation, and atresia
| [21] | Papadakis G, Hans D, Gonzalez Rodriguez E, et al. Menopausal hormone therapy is associated with reduced total and visceral adiposity: The osteolaus cohort. J Clin Endocrinol Metab. 2018; 103(5): 1948-1957.
https://doi.org/10.1210/jc.2017-02458 |
[21]
. Elevated androgen levels can inhibit the proliferation of ovarian granulosa cells, promote their apoptosis, and hinder oocyte growth and development, resulting in follicular development arrest and impaired kinetics
| [22] | Qi X, Zhang B, Zhao Y, et al. Hyperhomocysteinemia Promotes Insulin Resistance and Adipose Tissue Inflammation in PCOS Mice Through Modulating M2 Macrophage Polarization via Estrogen Suppression. [J]. Endocrinology, 2017, 158(10): 3591-3603. https://doi.org/10.1210/en.2017-00629 |
[22]
.
To further elucidate the diagnostic value of common clinical indicators for predicting pregnancy outcomes in patients with polycystic ovary syndrome (PCOS), this study employed Pearson correlation and Receiver Operating Characteristic (ROC) curve analyses across four distinct groups: the control group, PCOS group, polycystic ovary morphology (PCOM) group, and hyperandrogenism (HA) group. As detailed in Section 2.3, the results revealed a strong correlation between the fertilization rate and clinical indicators, including age, alanine aminotransferase (ALT), aspartate aminotransferase (AST), AST/ALT ratio, creatinine (Cr), urea nitrogen to creatinine ratio (UN/Cr), vaginal pH (V-PH), D-dimer (D-D), thyroid-stimulating hormone (TSH), and cancer antigen 125 (CA125). Similarly, a robust association was identified between the good embryo rate and the same clinical indicators.
To enhance the diagnostic precision of these correlations, Youden index analysis was performed on the aforementioned indicators. Notably, for fertilization rate, the clinical indicator Cr exhibited a Youden index greater than 0.50, suggesting that altered body pH associated with elevated creatinine levels may disrupt metabolic balance in PCOS patients. In terms of good embryo rate, the indicators Age, AST/ALT ratio, UN/Cr, D-D, and CA125 all demonstrated Youden indices exceeding 0.50. Based on the comprehensive findings of this study, Age, AST/ALT ratio, UN/Cr, D-D, CA125, and Cr can be regarded as predictive indicators for assessing pregnancy outcomes in PCOS patients, with respective cutoff values of 30.50, 1.15, 75.78, 289.00, 17.85, and 56.50.
Poor pregnancy outcomes associated with polycystic ovary syndrome (PCOS) represent a significant consequence of the disease's onset and progression in women of reproductive age
| [12] | Dapas M, Dunaif A. Deconstructing a Syndrome: Genomic Insights Into PCOS Causal Mechanisms and Classification. [J]. Endocr Rev, 2022, 43(6): 927-965.
https://doi.org/10.1210/endrev/bnac001 |
| [13] | Kazemi M, Kim JY, Wan C, et al. Comparison of dietary and physical activity behaviors in women with and without polycystic ovary syndrome: a systematic review and meta-analysis of 39 471 women. [J]. Hum Reprod Update, 2022, 28(6): 910-955. https://doi.org/10.1093/humupd/dmac023 |
[12, 13]
. Several studies propose that PCOS may originate in adolescence, marked by a gradual and ongoing development. Notably, clinical indicators in many PCOS patients—including inflammatory and endocrine markers such as liver function parameters, fasting blood glucose, and complete blood count, even including body mass index—may remain within normal ranges. This presents a considerable challenge for early detection and diagnosis in the initial stages of disease progression, often resulting in missed opportunities for timely intervention and subsequent severe infertility outcomes.
Our key finding is that subtle clinical indicators changes emerge with disease progression. The primary contribution of this research is the focus on identifying and assessing key clinical markers, as well as in refining their diagnostic value concerning pregnancy outcomes in PCOS. Continuous monitoring and management of these indicators, along with the observation of their trend changes, may prove more beneficial for assessing the condition of PCOS patients than relying solely on static indicator values.
In conclusion, for patients with polycystic ovary syndrome (PCOS), long-term health monitoring and trend analysis of key clinical indicators is essential, specifically Age, AST/ALT, UN/Cr, D-D, CA125, and Cr. provide better PCOS assessment than static values. Furthermore, their practicality and accessibility enhance their utility; the associated tests are cost-effective and straightforward to administer for both patients and healthcare institutions.
The implementation of these predictive indicators can markedly improve assessment capabilities within primary hospitals and clinics that do not specialize in obstetrics and gynecology. Such advancements could enable early screening of high-risk individuals for PCOS and facilitate timely interventions, thus reducing the likelihood of negative pregnancy outcomes.
Nevertheless, it is crucial to recognize the study's limitations, especially the limited sample size. Ongoing validate the predictive value of Age, AST/ALT, UN/Cr, D-D, CA125, and Cr in relation to PCOS disease activity, larger-scale studies are warranted.
Abbreviations
PCOS | Polycystic Ovary Syndrome |
PCOM | Polycystic Ovarian Morphology |
HA | Hyperandrogenism |
BMI | Body Mass Index |
DD / D-D | D-dimer |
ALT | Alanine Aminotransferase |
AST | Aspartate Aminotransferase |
Cr | Creatinine |
UN | Urea Nitrogen |
Glu | Fasting Plasma Glucose |
Fins / FIN | Fasting Insulin |
TSH | Thyroid-Stimulating Hormone |
WBC | White Blood Cell |
ESR | Erythrocyte Sedimentation Rate |
Gran | Absolute Neutrophil Count |
Gran% | Neutrophil Percentage |
V-PH | Vaginal pH |
CA125 | Cancer Antigen 125 |
MAFLD | Metabolic Associated Fatty Liver Disease |
HIS | Hepatic Insulin Sensitivity Score |
BARD | Body Mass Index, AST/ALT Ratio, Diabetes Score |
ROC | Receiver Operating Characteristic |
AUC | Area Under the Curve |
YI | Youden’s Index |
NHS | National Health Service |
GnRH | Gonadotropin-Releasing Hormone |
IL | Interleukin |
TNF-α | Tumor Necrosis Factor-alpha |
CCL2 | C-C Motif Chemokine Ligand 2 |
iNOS | Inducible Nitric Oxide Synthase |
hsCRP | High-Sensitivity C-Reactive Protein |
FFA | Free Fatty Acid |
SPSS | Statistical Package for the Social Sciences |
AMH | Anti-Müllerian Hormone |
GLUT4 | Glucose Transporter Type 4 |
Author Contributions
Tianyuan Pan: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing
Chuyan Li: Data curation, Formal Analysis, Methodology, Resources, Software, Writing – original draft
Funding
Zhejiang Provincial Natural Science Foundation (LQ21H090014), Zhejiang Provincial Medical and Health Research Project (2022RC025), Zhejiang University Interdisciplinary Preliminary Research Project (S20220187), The opening foundation of the State Key Laboratory for Diagnosis and Treatment of Infectious Diseases, The First Affiliated Hospital, Zhejiang University School of Medicine (SKLID2022KF04).
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Ioannis G, Lempesis, Samuel J, Apple, Gustavo, Duarte et al. Cardiometabolic effects of SGLT2 inhibitors on polycystic ovary syndrome. [J]. Diabetes Metab Res Rev, 2023, 39: e3634.
https://doi.org/10.1002/dmrr.3634
|
| [2] |
Anastasia, Trouva, Michael, Alvarsson, Jan, Calissendorff et al. Maternal thyroid function and offspring birth anthropometrics in women with polycystic ovary syndrome. [J]. Front Endocrinol (Lausanne), 2024, 15: 1343277.
https://doi.org/10.3389/fendo.2024.1343277
|
| [3] |
Cesta CE, Öberg AS, Ibrahimson A, et al. Maternal polycystic ovary syndrome and risk of neuropsychiatric disorders in offspring: Prenatal androgen exposure or genetic confounding?. Psychol Med. 2020; 50(4): 616-624.
https://doi.org/10.1017/S0033291719000424
|
| [4] |
Wu Q, Gao J, Bai D, Yang Z, Liao Q. The prevalence of polycystic ovarian syndrome in Chinese women: A meta-analysis. Ann Palliat Med. 2021; 10(1): 74-87.
https://doi.org/10.21037/apm-20-1881
|
| [5] |
David H, Abbott, Daniel A, Dumesic. Monoclonal antibody therapy for PCOS? [J]. Cell Metab, 2025, 37(2): 211-213.
https://doi.org/10.1016/j.cmet.2024.12.009
(Note: 2025 article, verify upon publication).
|
| [6] |
Cotellessa L, Sobrino V, Silva MSB, et al. Preventing and correcting polycystic ovary syndrome by targeting anti-Müllerian hormone signaling in minipuberty and adulthood in mice. [J]. Cell Metab, 2025, 37(2): 248-262. e6.
https://doi.org/10.1016/j.cmet.2024.11.013
|
| [7] |
Stener-Victorin E, Padmanabhan V, Walters KA, et al. Animal Models to Understand the Etiology and Pathophysiology of Polycystic Ovary Syndrome. [J]. Endocr Rev, 2020, 41(4): bnaa010.
https://doi.org/10.1210/endrev/bnaa010
|
| [8] |
Fischer MB, Mola G, Rom AL, et al. Ovarian and Uterine Morphology in Minipuberty: Associations With Reproductive Hormones: a COPANA Study of 302 Girls. J Clin Endocrinol Metab. 2025; 110(4): 1015-1022.
https://doi.org/10.1210/clinem/dgad738
|
| [9] |
Abbott DH, Levine JE, Dumesic PA, et al. POLYCYSTIC OVARY SYNDROME: ORIGINS AND IMPLICATIONS: Gestational anti-Müllerian hormone and testosterone excess combined with maternal adiposity program for polycystic ovary syndrome. [J]. Reproduction, 2025, 170(1): R1-R12.
https://doi.org/10.1530/REP-23-0548
|
| [10] |
Joham AE, Norman RJ, Stener-Victorin E, et al. Polycystic ovary syndrome. Lancet Diabetes Endocrinol. 2022; 10(9): 668-680.
https://doi.org/10.1016/S2213-8587(22)00163-2
|
| [11] |
di Clemente N, Racine C, Pierre A, et al. Anti-Müllerian Hormone in Female Reproduction. [J]. Endocr Rev, 2021, 42(6): 753-782.
https://doi.org/10.1210/endrev/bnab012
|
| [12] |
Dapas M, Dunaif A. Deconstructing a Syndrome: Genomic Insights Into PCOS Causal Mechanisms and Classification. [J]. Endocr Rev, 2022, 43(6): 927-965.
https://doi.org/10.1210/endrev/bnac001
|
| [13] |
Kazemi M, Kim JY, Wan C, et al. Comparison of dietary and physical activity behaviors in women with and without polycystic ovary syndrome: a systematic review and meta-analysis of 39 471 women. [J]. Hum Reprod Update, 2022, 28(6): 910-955.
https://doi.org/10.1093/humupd/dmac023
|
| [14] |
Geng L, Yang X, Sun J, et al. Gut Microbiota Modulation by Inulin Improves Metabolism and Ovarian Function in Polycystic Ovary Syndrome. [J]. Adv Sci (Weinh), 2025, 12(8): e2308401.
https://doi.org/10.1002/advs.202308401
|
| [15] |
Martínez-García MÁ, Luque-Ramírez M, San-Millán JL, et al. Body iron stores and glucose intolerance in premenopausal women: role of hyperandrogenism, insulin resistance, and genomic variants related to inflammation, oxidative stress, and iron metabolism. [J]. Diabetes Care, 2009, 32(5): 934-936.
https://doi.org/10.2337/dc08-1962
|
| [16] |
Chen YH, Heneidi S, Lee JM, et al. miRNA-93 inhibits GLUT4 and is overexpressed in adipose tissue of polycystic ovary syndrome patients and women with insulin resistance. Diabetes. 2013; 62(7): 2278-2286.
https://doi.org/10.2337/db12-0963
|
| [17] |
Ambikairajah A, Walsh E, Tabatabaei-Jafari H, Cherbuin N. Fat mass changes during menopause: a meta-analysis. Am J Obstet Gynecol. 2019; 221(5): 393-409.
https://doi.org/10.1016/j.ajog.2019.04.023
|
| [18] |
Xiao Peng, Ren Jingjing, Yao Lingnu, et al. Longitudinal study of chronic low-grade inflammatory response in polycystic ovary syndrome: preliminary compilation and analysis of inflammation and related endocrine risk indicators [J]. General Practice Clinical and Education, 2021, 19(02): 102-107.
|
| [19] |
Torstensson S, Ascani A, Risal S, et al. Androgens Modulate the Immune Profile in a Mouse Model of Polycystic Ovary Syndrome. [J]. Adv Sci (Weinh), 2024, 11(5): e2304470.
https://doi.org/10.1002/advs.202304470
|
| [20] |
Lang Q, Yang Y, Zhang X, et al. Etanercept-mediated anti-TNF-α therapy ameliorates the phenotype of PCOS model induced by letrozole. PLoS One. 2019; 14(6): e0217495.
https://doi.org/10.1371/journal.pone.0217495
|
| [21] |
Papadakis G, Hans D, Gonzalez Rodriguez E, et al. Menopausal hormone therapy is associated with reduced total and visceral adiposity: The osteolaus cohort. J Clin Endocrinol Metab. 2018; 103(5): 1948-1957.
https://doi.org/10.1210/jc.2017-02458
|
| [22] |
Qi X, Zhang B, Zhao Y, et al. Hyperhomocysteinemia Promotes Insulin Resistance and Adipose Tissue Inflammation in PCOS Mice Through Modulating M2 Macrophage Polarization via Estrogen Suppression. [J]. Endocrinology, 2017, 158(10): 3591-3603.
https://doi.org/10.1210/en.2017-00629
|
Cite This Article
-
-
@article{10.11648/j.cmr.20251406.14,
author = {Tianyuan Pan and Chuyan Li},
title = {Association of Common Clinical Indicators with Pregnancy Outcomes in Polycystic Ovary Syndrome (PCOS)},
journal = {Clinical Medicine Research},
volume = {14},
number = {6},
pages = {229-237},
doi = {10.11648/j.cmr.20251406.14},
url = {https://doi.org/10.11648/j.cmr.20251406.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.cmr.20251406.14},
abstract = {Objective This study seeks to explore the association between common clinical indicators and pregnancy outcomes in patients with polycystic ovary syndrome (PCOS). Methods A cohort of 52 women with PCOS, 22 with isolated polycystic ovarian morphology (PCOM), 13 with isolated hyperandrogenism (HA), and 59 healthy controls was recruited from the Department of Reproductive Medicine, First Affiliated Hospital, Zhejiang University School of Medicine, between June 2021 and September 2022. Clinical parameters including age and body mass index (BMI) were recorded, while levels of D-dimer (DD), alanine aminotransferase (ALT), aspartate transaminase (AST), creatinine (Cr), urea nitrogen (UN), fasting plasma glucose (Glu), fasting insulin (Fins), and thyroid-stimulating hormone (TSH), embryo availability rate, fertilization Rate were measured. Differences across PCOS, PCOM, and HA groups were analyzed using analysis of variance and non-parametric tests. Results (1) In the PCOS group, significant differences were observed for embryo availability rate, age, WBC, TSH, ALT, AST, MAFLD, and BARD scores (P Conclusion Endocrine profiles differ significantly among PCOS, PCOM, and HA groups, and markers such as Age, ALT, AST, AST/ALT ratio, Cr, UN/Cr, DD, TSH, and CA125 can serve as potential predictors of pregnancy outcomes in patients with PCOS.},
year = {2025}
}
 Copy
|
Copy
|
 Download
Download
-
TY - JOUR
T1 - Association of Common Clinical Indicators with Pregnancy Outcomes in Polycystic Ovary Syndrome (PCOS)
AU - Tianyuan Pan
AU - Chuyan Li
Y1 - 2025/12/29
PY - 2025
N1 - https://doi.org/10.11648/j.cmr.20251406.14
DO - 10.11648/j.cmr.20251406.14
T2 - Clinical Medicine Research
JF - Clinical Medicine Research
JO - Clinical Medicine Research
SP - 229
EP - 237
PB - Science Publishing Group
SN - 2326-9057
UR - https://doi.org/10.11648/j.cmr.20251406.14
AB - Objective This study seeks to explore the association between common clinical indicators and pregnancy outcomes in patients with polycystic ovary syndrome (PCOS). Methods A cohort of 52 women with PCOS, 22 with isolated polycystic ovarian morphology (PCOM), 13 with isolated hyperandrogenism (HA), and 59 healthy controls was recruited from the Department of Reproductive Medicine, First Affiliated Hospital, Zhejiang University School of Medicine, between June 2021 and September 2022. Clinical parameters including age and body mass index (BMI) were recorded, while levels of D-dimer (DD), alanine aminotransferase (ALT), aspartate transaminase (AST), creatinine (Cr), urea nitrogen (UN), fasting plasma glucose (Glu), fasting insulin (Fins), and thyroid-stimulating hormone (TSH), embryo availability rate, fertilization Rate were measured. Differences across PCOS, PCOM, and HA groups were analyzed using analysis of variance and non-parametric tests. Results (1) In the PCOS group, significant differences were observed for embryo availability rate, age, WBC, TSH, ALT, AST, MAFLD, and BARD scores (P Conclusion Endocrine profiles differ significantly among PCOS, PCOM, and HA groups, and markers such as Age, ALT, AST, AST/ALT ratio, Cr, UN/Cr, DD, TSH, and CA125 can serve as potential predictors of pregnancy outcomes in patients with PCOS.
VL - 14
IS - 6
ER -
Copy
|
Download